
Medication-Induced Psychosis Risk Assessment Tool
Medication Safety Assessment
This tool helps you identify potential risk of medication-induced psychosis. Note: This is for informational purposes only. Always consult your healthcare provider.
Risk Assessment Results
When someone suddenly starts seeing things that aren’t there, believing they’re being watched, or speaking in ways that make no sense, it’s easy to assume it’s schizophrenia or another mental illness. But what if the cause isn’t their brain wiring-it’s a pill they took yesterday?
Medication-induced psychosis is more common than most people realize. It’s not rare. It’s not exotic. It’s a real, documented reaction to everyday drugs-steroids, antibiotics, even over-the-counter sleep aids. And when it happens, it’s an emergency that needs fast, smart action.
What Medication-Induced Psychosis Actually Looks Like
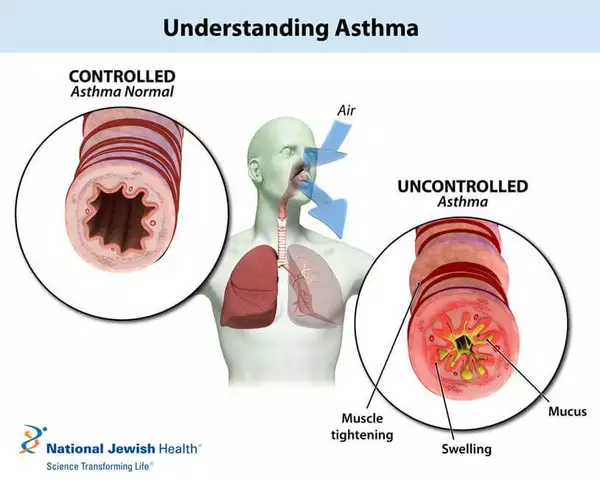
It starts quietly. A patient on high-dose prednisone for asthma starts feeling uneasy. Then they’re convinced their neighbor is stealing their mail. Then they hear voices whispering their name. A person taking malaria pills for a trip to Southeast Asia begins pacing at night, muttering about invisible enemies. Someone on a new antidepressant suddenly can’t sleep, feels paranoid, and claims their phone is broadcasting their thoughts.
These aren’t just bad side effects. They’re full-blown psychotic symptoms: delusions, hallucinations, disorganized speech, and a loss of touch with reality. The most common signs are:
- Delusions: False beliefs that stick even when proven wrong-like being followed, poisoned, or controlled by outside forces.
- Hallucinations: Hearing voices, seeing shadows move, feeling bugs crawl under the skin. Auditory hallucinations are the most frequent.
- Disorganized thinking: Jumping between unrelated topics, speaking incoherently, or repeating phrases.
- Agitation or withdrawal: Sudden aggression, pacing, or shutting down completely.
- Memory and focus problems: Forgetting where they are, unable to follow simple instructions.
It’s not always obvious. Sometimes anxiety, irritability, or insomnia shows up first-like a warning sign before the full episode hits. This is especially true with steroids or antimalarials. If someone’s mood shifts sharply after starting a new medication, don’t ignore it.
Which Medications Can Trigger This?
It’s not just street drugs. Prescription and even OTC meds can do this. Here are the top culprits:
- Corticosteroids: Prednisone, dexamethasone. Up to 5.7% of people on high doses develop psychosis. It’s one of the most common drug-induced causes.
- Antimalarials: Mefloquine. The European Medicines Agency has logged over 1,200 psychosis cases since 1985. Travelers often don’t realize the risk until it’s too late.
- Antiretrovirals: Efavirenz (used for HIV). About 2.3% of users report hallucinations or severe anxiety. The FDA requires warning labels.
- Antidepressants: SSRIs and SNRIs. Rare, but documented. Often happens in the first few weeks, especially in people with no prior mental health history.
- Stimulants: Methylphenidate, amphetamines. Used for ADHD, but high doses can trigger paranoia and hallucinations.
- Anticholinergics: Diphenhydramine (Benadryl), some sleep aids. Especially dangerous in older adults.
- Levodopa and dopamine agonists: For Parkinson’s. Can cause vivid dreams turning into full hallucinations.
- Opioids and NSAIDs: In high doses or with kidney/liver problems, even ibuprofen or oxycodone can cause confusion and delusions.
And yes-cannabis. Up to 10% of users experience psychotic symptoms. Methamphetamine? Over 11% of users. Cocaine? Nearly 96% of heavy users report hallucinations. But here’s the key: if the symptoms stop when the drug wears off, it’s not psychosis. It’s intoxication. True medication-induced psychosis means the symptoms keep going after the drug is out of the system.
How to Tell It’s Not Schizophrenia
This is the biggest mistake doctors make. Mistaking drug-induced psychosis for schizophrenia leads to lifelong antipsychotic prescriptions-when the real fix is just stopping the drug.
The DSM-5 says: if psychotic symptoms start during or within a month of taking a drug (or withdrawing from it), and they go away after the drug is stopped, it’s medication-induced. If they stick around longer than a month, then you look at primary disorders.
But it’s messy. Many people have both. A 2023 study found 74% of first-episode psychosis patients had a history of substance use. So how do you know?
- Timing matters: Did symptoms start within days of a new med? Likely drug-induced.
- History matters: No prior psychosis? No family history? Then drug-induced is more likely.
- Symptom profile: Steroid psychosis often includes mood swings and confusion. Stimulant psychosis is usually paranoid with visual hallucinations.
- Recovery speed: Cocaine psychosis clears in 1-3 days. Steroid psychosis takes 4-6 weeks. Schizophrenia doesn’t fade on its own.
Doctors need to ask: What did you start taking in the last 30 days? Not just prescriptions-supplements, herbal teas, sleep aids, even cough syrup. Many patients forget to mention these.
What to Do in an Emergency
If someone is actively hallucinating, terrified, or threatening harm to themselves or others-call 911 or go to the ER. Don’t wait. Don’t try to reason with them. They’re not being difficult. Their brain is malfunctioning.
Emergency teams follow a clear protocol:
- Stop the drug: The #1 treatment. No exceptions. If it’s a steroid, they’ll start tapering it. If it’s an illicit stimulant, they’ll monitor withdrawal.
- Stabilize: IV fluids, electrolytes, check for rhabdomyolysis (muscle breakdown from stimulants), monitor heart rate and temperature.
- Manage symptoms: If the person is violent or in extreme distress, low-dose atypical antipsychotics like olanzapine or quetiapine are given. But only if needed. Not as a first-line fix.
- Rule out other causes: Blood tests for infections, thyroid issues, liver failure, or vitamin B1 deficiency (Wernicke-Korsakoff from chronic alcohol use).
For alcohol or benzo withdrawal psychosis, they use benzodiazepines-slowly-to prevent seizures and delirium tremens. For stimulant overdose, they use cooling, fluids, and sometimes sedation.
And yes-in severe cases, involuntary hold is legal. If someone is a danger to themselves or others, hospitals can detain them for 72 hours under mental health laws. This isn’t punishment. It’s protection.
Recovery and What Comes After
Most people get better. Fast.
Cocaine-induced psychosis? Usually gone in 72 hours. Steroid psychosis? Clears in 4-6 weeks. Antidepressant-triggered? Often resolves within 1-2 weeks of stopping.
But here’s the catch: some don’t. If symptoms linger past a month, you’re looking at a possible underlying disorder. That’s why follow-up is non-negotiable.
After the crisis, patients need:
- Psychiatric evaluation: To confirm whether this was a one-time reaction or a sign of something deeper.
- Medication review: Every single drug-prescription, OTC, supplement-needs to be re-evaluated.
- Education: Patients and families need to know: Don’t restart this drug. Ever. Even a small dose can trigger it again.
- Monitoring for 3 months: The American Psychiatric Association recommends this. Relapse into primary psychosis can happen if you miss it.
And if someone had a reaction to a common drug like prednisone? They should never get it again. Not even for a short course. The risk is too high.
How to Prevent It
Prevention starts with awareness.
- Ask before prescribing: Doctors should screen for personal or family history of psychosis, bipolar disorder, or substance abuse before starting high-risk meds like steroids, antimalarials, or efavirenz.
- Warn patients: FDA-mandated patient guides for drugs like efavirenz say: Call your doctor immediately if you feel depressed, anxious, or hear voices. That advice should be standard for all high-risk drugs.
- Watch the first few weeks: That’s when most reactions happen. If someone’s mood drops, they’re restless, or sleeping poorly after a new med-don’t brush it off.
- Check OTC and supplements: Benadryl, energy drinks, weight-loss pills, even melatonin can trigger psychosis in sensitive people.
And if you’re the patient? Keep a list of everything you take. Every pill, drop, or powder. Bring it to every appointment. Say: “I’ve been feeling off since I started this. Could it be the meds?” Most doctors won’t ask. You have to.
Bottom Line
Medication-induced psychosis isn’t a myth. It’s not rare. It’s not always obvious. But it’s treatable-if you catch it fast.
It’s not about blaming the drug. It’s about recognizing that medication-induced psychosis can happen to anyone, anytime. A healthy person on a common steroid. An elderly patient on Benadryl. A young adult with ADHD on stimulants.
The fix isn’t more therapy. It’s not lifelong pills. It’s stopping the trigger-and acting before it escalates.
If you or someone you know suddenly loses touch with reality after starting a new medication-don’t wait. Don’t hope it goes away. Call a doctor. Go to the ER. It could save their life.




December 8, 2025 AT 07:56
Desmond Khoo
Bro this hit different. My aunt went full-on ‘I’m being watched by the microwave’ after her steroid shot for allergies. We thought it was dementia until the doctor asked about meds. 🤯 She’s fine now, but man-never underestimate a pill. Save this post for your next doctor visit.
December 10, 2025 AT 06:10
Sadie Nastor
i just read this and cried a little. my cousin took benadryl for allergies and started screaming about spiders in her eyes… for 3 days. no one believed us until we showed the label. 🫂 please, if you’re on anything new and feel ‘off’-trust yourself. you’re not crazy. the drug might be.
December 11, 2025 AT 11:15
Kyle Flores
This is the kind of info every ER nurse and primary doc needs to print and tape to their desk. I’ve seen too many people get labeled ‘schizophrenic’ after a bad reaction to prednisone or efavirenz. They get locked into antipsychotics for life when all they needed was to stop the pill.
And honestly? The fact that OTC meds like diphenhydramine can do this? That’s wild. My grandma took 4 Benadryl to sleep and thought her TV was talking to her. She’s 82. No prior history. Just old body + wrong pill.
Doctors need to ask ‘what did you start?’ not ‘what’s wrong with you?’
December 12, 2025 AT 23:56
Olivia Hand
Let’s talk about the elephant in the room: the pharmaceutical industry’s silence on this. They slap a tiny warning in the 12-point font at the bottom of the insert, but never train prescribers to recognize the early red flags.
And why? Because if they did, people would stop taking the drugs. And money? Money talks louder than minds.
But here’s the kicker-most of these reactions are dose-dependent and reversible. So why not screen for genetic susceptibility? Why not test for CYP450 enzyme variants before prescribing? We have the tech. We just don’t care enough.
Until we treat psychiatric side effects like we treat liver toxicity, people will keep getting misdiagnosed. And that’s not negligence-it’s negligence with a profit margin.
December 13, 2025 AT 15:40
Louis Llaine
So… you’re telling me the same meds that make my ADHD brain stop screaming can also make me think my toaster is plotting against me? Cool. I’ll just take my Adderall and pray to the algorithm. 🤡
December 14, 2025 AT 15:40
Jane Quitain
thank you for writing this!! i was so scared when my boyfriend started hearing voices after his new sleep aid… i thought he was cheating on me or something 😅 but then i found this article and we went to the ER. they said it was melatonin + diphenhydramine combo. he’s back to normal now. never again. 💙
December 15, 2025 AT 03:48
Sam Mathew Cheriyan
lol they don’t want you to know this but 90% of ‘psychosis’ is actually government mind control via 5G and fluoridated water. the meds are just a distraction. they give you antipsychotics to keep you quiet while they sync your thoughts to satellites. my cousin took steroids and started seeing ‘the grid’-that’s not psychosis, that’s him waking up. 🛰️👁️
December 15, 2025 AT 23:40
Ernie Blevins
So what? People take drugs. They get weird. Big deal. Just lock them up. Problem solved. 🤷♂️