
Picture this: almost one in three adults worldwide deals with high cholesterol. It's the silent risk factor sneaking into our arteries, setting us up for heart attacks and strokes. Doctors have turned to statins for decades as their first line of defense. But with so many brands out there—Zocor (simvastatin), Lipitor (atorvastatin), Crestor (rosuvastatin)—how do you decide what's actually right for you? On top of that, what if you can't tolerate statins at all? Believe it or not, the answer isn’t as simple as picking the “strongest” pill. There are some key differences that can make or break your experience—from how the drug works in your liver to the way your everyday lifestyle might tip the scales.
Understanding Simvastatin (Zocor): How It Works and Who It Helps
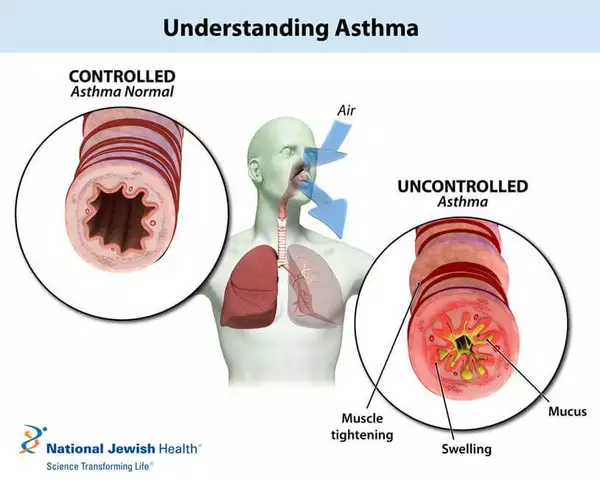
Simvastatin, better known by its brand name Zocor, belongs to the statin family. Statins suppress a liver enzyme called HMG-CoA reductase, which the body uses to make cholesterol. Less enzyme activity means lower cholesterol production. Over time, your numbers usually drop—sometimes fast enough for you to notice on your next blood test. But simvastatin isn't just a one-size-fits-all solution. Its main edge? Affordability and a long track record. It's been around since the late 1980s and is available as a generic drug, which means you’re less likely to get sticker shock at the pharmacy.
But here's the deal—while simvastatin is tried and true, it's not always the safest at high doses. Studies from as early as 2011 flagged that muscle pain and even a rare issue called rhabdomyolysis become a bigger risk if you go above 40 mg per day. Doctors now usually start patients at lower doses and often look to other statins if high-potency cholesterol lowering is needed. That doesn't mean simvastatin doesn't work. For folks with moderately high cholesterol or those on a tight budget, it can be a real game-changer. But don’t overlook that simvastatin can interact with other meds—especially certain antibiotics, antifungals, and even grapefruit juice. It’s worth reading through a straight-up guide to Zocor uses and what else to know before you fill your script.
Comparing Zocor, Lipitor, and Crestor: Potency, Side Effects, and Flexibility
Not all statins pack the same punch. Atorvastatin (Lipitor) and rosuvastatin (Crestor) are newer, stronger, and more flexible with dosing. What does that mean on the ground? If your cholesterol levels are sky-high, these two pull double duty: they lower LDL (the “bad” cholesterol) and often do more for bumping up HDL (“good” cholesterol). A head-to-head study published in the New England Journal of Medicine found that high-dose atorvastatin cut LDL cholesterol by about 50%, compared to simvastatin's 35% at standard doses. Rosuvastatin, even at moderate doses, sometimes beats both for stubbornly high readings.
Side effects? Above all, statins have a reputation for muscle aches. While simvastatin is notorious for this at higher doses, Lipitor and Crestor are less likely to tip you into serious muscle issues even when you need more firepower. That said, any statin can cause trouble for a small percentage. They might nudge up liver enzymes or (rarely) mess with blood sugar, especially if you already have diabetes risks. Atorvastatin and rosuvastatin, though, are less likely to be affected by food—simvastatin needs to be taken in the evening for max effect, but the other two? You can take them pretty much any time, even with dinner.
| Statin | Best For | LDL Lowering (% Approx.) | Common Dose Range (mg) | Major Side Effect Risk |
|---|---|---|---|---|
| Simvastatin (Zocor) | Budget, Modest LDL targets | 35-40% | 10-40 | Muscle issues at high doses |
| Atorvastatin (Lipitor) | High LDL, Flexible dosing | 39-60% | 10-80 | Mild blood sugar increase |
| Rosuvastatin (Crestor) | Very high LDL, High-risk patients | 45-63% | 5-40 | Muscle aches, rare kidney concerns |
Insurance can sway your pick too. Simvastatin is almost always the cheapest with or without coverage. Lipitor and Crestor are both generic now, but some plans still put them behind higher copays. Age and ethnicity also play a role—Asians for example may need lower rosuvastatin doses, because their bodies absorb more of the drug. And for people who hate popping pills, atorvastatin and rosuvastatin work longer in your bloodstream. Some docs even suggest alternate-day dosing if side effects crop up.
When Statins Aren’t for You: Exploring Non-Statin Alternatives
So, what if statins cause you nothing but grief—achy, tired, or just plain miserable? Luckily, you aren’t out of options. Several non-statin cholesterol medications have come to the rescue in the past decade. Ezetimibe (Zetia) is the front runner. It doesn’t block production; instead, it messes with how your intestines soak up cholesterol from food. On average, it drops LDL by 13-20% and often gets paired with a low-dose statin for more impact with less risk of muscle pain.
If your LDL levels just won’t budge, even on maximum statins, doctors may talk about PCSK9 inhibitors like alirocumab (Praluent) or evolocumab (Repatha). These are injectables, not pills. They work by unlocking the body’s natural ability to recycle and clear LDL cholesterol from the blood. In big clinical trials, patients cut their LDL by up to 60% even with family histories of sky-high numbers. Downside? They’re expensive and not usually first pick unless you’re at extreme heart risk.
Other options include bile acid sequestrants, which grab cholesterol in your gut, and niacin, a type of vitamin B that hit the market before statins. The problem is they often bring their own set of stomach or flushing side effects, and recent data says they don’t reduce heart attacks quite as well. One less talked-about newcomer: bempedoic acid (Nexletol). It's another oral drug that blocks cholesterol in the liver, with a lower risk of muscle troubles, though real-world results are still coming in.
Then there are the old favorites: eating more fiber, especially from oats and beans, and adding plant sterols or stanols. These natural cholesterol-busters, when used with meds or even by themselves, can lower LDL by another 10%. Walking just 30 minutes per day, five times a week, is proven to help. If you smoke, quitting gives your HDL cholesterol a boost almost immediately—it’s like a free medication with no copay.
Tips for Switching Cholesterol Medicine: What Doctors Don’t Always Tell You
Switching from one cholesterol med to another can feel like jumping into unknown waters. Most people start because they get side effects or their cholesterol just won’t budge. The key is knowing transitions aren’t always straight swaps. For example, switching from simvastatin to atorvastatin isn’t just milligram for milligram. Atorvastatin is more potent, so you’ll probably need a lower dose by number, but get stronger LDL reduction.
Here's a pro tip: if your insurance switches your brand by default or the pharmacy gives you a new generic, check the pill color and name. Mix-ups confuse everyone and even small mistakes matter here. If your doctor is switching you due to muscle issues, ask about taking a week off before starting a new statin. This “washout” helps your body reset and lets you see what the drug is actually doing once you restart.
Lab monitoring matters more than you think. Most people need a cholesterol check about eight weeks after any change. If you’re on high-dose statins and over age 70, mention any unexpected pains, especially if you start a new antibiotic or antifungal. These meds can turbocharge statins in your system and push muscle side effects through the roof.
- Keep a daily symptom diary for the first two months of any medication change.
- Bring it to your follow-up visit—the details can catch subtle drug reactions before they get serious.
- Don’t skip your cholesterol labs, even if you feel fine. Some side effects show up in bloodwork before you ever notice anything yourself.
If you’re worried about muscle side effects, ask about alternate-day dosing or trying CoQ10, a supplement that may cut the risk (though the evidence still isn’t crystal clear). And if a doctor shrugs off your concerns, remember: your lived experience matters. You know your body best.

FAQ: Simvastatin and Its Alternatives in Real Life
What about mixing statins with other popular drugs like blood pressure meds? Totally common. Most statins mix safely with ACE inhibitors and beta-blockers, but always check for weird interactions. How long do you need to take these meds? Most people stay on them for life, but if you lose a lot of weight or change your diet dramatically, doses might go down over time. Is there a “right” age to start? Heart risk—not age alone—guides the choice. Teens and people in their twenties with sky-high inherited cholesterol sometimes need statins, but most patients start after 40, when risk really starts to climb.
Here’s a wild fact: classic statins like Zocor have saved millions of lives globally, but up to 30% of people don’t reach their LDL cholesterol targets on their first statin. That’s why having more than one option matters so much. For those hunting for alternatives, remember that non-statin meds aren’t magic bullets—they work best paired with lifestyle changes.
One last thought—if you’re worried about statin-induced diabetes risk, recent major studies suggest the increase is real, but pretty small—about one extra case per 1,000 people per year. If you already have risk factors, pay extra attention to blood sugar, and don’t ignore the simple stuff like diet tweaks and movement.
So does simvastatin win out over its cousins or is a non-statin in your future? It depends on your targets, your body, and how you react to treatment. Don’t be afraid to bring up what you read here with your doctor—it could change your care for the better.






July 25, 2025 AT 20:23
Jenni Waugh
Let’s be real-Zocor is the pharmaceutical equivalent of a flip phone in a world of iPhones. Sure, it ‘works,’ but why are we still pretending it’s the best option for anyone with actual cholesterol numbers above ‘mildly inconvenient’? If you’re on simvastatin and still hitting 160 LDL, you’re not being proactive-you’re just budgeting for a heart attack. And don’t even get me started on grapefruit juice. That’s not a breakfast companion, that’s a medical liability. Someone’s gotta say it: if your doctor still prescribes this like it’s 2005, they’re either lazy or getting kickbacks from the generic manufacturer.
July 26, 2025 AT 02:02
Jacqueline Anwar
The assertion that simvastatin is ‘affordable’ is technically accurate, yet morally bankrupt. When one considers the downstream costs of rhabdomyolysis, hospitalization, and subsequent statin intolerance, the ‘savings’ evaporate into a void of iatrogenic harm. Moreover, the comparative efficacy data presented is statistically sound, yet ethically incomplete: it fails to account for interindividual pharmacokinetic variance, particularly in CYP3A4 polymorphisms, which disproportionately affect patients of African descent. To recommend simvastatin as a first-line agent without genetic screening is not clinical practice-it is negligence dressed in white coats.
July 26, 2025 AT 08:11
Ganesh Kamble
bro why are we even talking about this? statins are just big pharma’s way of making you pay for water. just eat less meat and walk more. also i took zocor once and felt like a zombie for a week. no thanks.
July 28, 2025 AT 00:10
Theresa Ordonda
Okay but can we talk about how everyone ignores the real villain here? 😤 It’s not the meds-it’s the fact that we’re told to take a pill instead of fixing our diets. I’ve seen people on Crestor eating donuts for breakfast like it’s a lifestyle choice. 🤦♀️ CoQ10? Please. Eat more kale. Walk. Stop drinking soda. No pill fixes a 30-year habit of processed food. And if your doctor doesn’t ask you about your fridge? Find a new one. 💪
July 28, 2025 AT 12:51
chantall meyer
I find the entire discourse reductive. The body is not a spreadsheet. Cholesterol is not a villain. The obsession with LDL as a metric is a cultural artifact of Western medicine’s reductionist tendencies. Lifestyle? Of course. But to reduce human physiology to a number on a lab slip is to misunderstand the very nature of health.
July 29, 2025 AT 19:13
Will RD
i switched from zocor to lipitor and my muscles stopped screaming. also i took it in the morning and didnt care about grapefruit. my doc said it was fine. so maybe stop overthinking it? just take the pill and move on.
July 29, 2025 AT 19:35
Samuel Wood
It’s fascinating how the article romanticizes ‘lifestyle changes’ while ignoring the structural barriers to dietary adherence-food deserts, wage stagnation, and the industrialization of nutrition. To suggest that ‘eating more fiber’ is a viable alternative for a single mother working two jobs is not just naive-it’s classist. The real issue isn’t patient compliance. It’s that we’ve outsourced public health to individual willpower while corporations profit from the resulting disease.